
ABSTRACT
The COVID-19 pandemic and corresponding measures impacted the organisation of services for abortion on request in Flanders, Belgium. This study describes abortion centre staff’s perceptions of the influence of protective measures on abortion consultations and procedures, and aims to identify obstacles and opportunities that arose from this situation. Through the anonymised patient records of one Flemish abortion centre, we compared the number of requests and abortions during the first lockdown (16 March–14 June 2020) with the same period in the five preceding years. Using a phenomenological approach, we documented the procedures and conducted interviews (all inductively coded in Nvivo) with the centre’s coordinator, seven psychosocial staff members and three doctors. Though fewer people requested and had an abortion, the pressure on the staff was high due to changed procedures. A substantial change was the substitution of telephone for in-person consultations, which the staff perceived as less suited for discussing worries, contraception counselling, and building trust. The centre remained accessible, but the staff perceived an influence on the emotional reactions of clients. Staff agreed that the lockdown did not negatively influence the abortion procedure itself. However, they felt a negative influence on the level of psychological support they could offer, especially in interactions with clients who were less certain of their choice and clients with whom there was no common language. When the lockdown was relaxed, a triage system was set up to ensure emotionally safe abortion care – as perceived by staff – for all clients.
Résumé
La pandémie de COVID-19 et les mesures correspondantes ont eu des répercussions sur l’organisation des services d’avortement à la demande en Flandre, Belgique. Cette étude décrit la façon dont le personnel des centres d’avortement voit l’influence des mesures protectrices sur les consultations et les procédures d’avortement, et souhaite identifier les opportunités et les obstacles créés par cette situation. À partir des dossiers anonymisés de patientes d’un centre d’avortement flamand, nous avons comparé le nombre de demandes et d’avortements pendant le premier confinement (16 mars – 14 juin 2020) avec la même période au cours d’années précédentes. À l’aide d’une approche phénoménologique, nous avons documenté les procédures et mené des entretiens (tous codés inductivement sur Nvivo) avec le coordonnateur du centre, sept membres du personnel psychosocial et trois médecins. Même si moins de personnes ont demandé et obtenu un avortement, la pression sur le personnel était élevée en raison du changement de procédure. L’une des modifications substantielles a été le remplacement des consultations en personne par des conversations téléphoniques, moins adaptées, de l’avis du personnel, pour parler des inquiétudes, conseiller sur la contraception et instaurer la confiance. Le centre est resté accessible, mais le personnel a perçu une influence sur les réactions émotionnelles des clients. Les membres du personnel ont convenu que le confinement n’avait pas eu de conséquences négatives sur la procédure d’avortement elle-même. Néanmoins, ils ont ressenti une influence négative sur le niveau de soutien psychologique qu’ils étaient en mesure d’offrir, spécialement dans les interactions avec les clientes qui étaient moins sûres de leur choix et les clientes avec lesquelles il n’y avait pas de langue commune. Après la levée du confinement, un système de triage a été établi pour garantir des soins pour avortement sûr du point de vue émotionnel, selon le jugement du personnel, pour toutes les clientes.
Resumen
La pandemia por COVID-19 y medidas correspondientes impactaron la organización de servicios de aborto a petición en Flandes, Bélgica. Este estudio describe las percepciones del personal del centro de aborto sobre la influencia de medidas protectoras relacionadas con consultas y procedimientos de aborto, y pretende identificar los obstáculos y las oportunidades que surgieron de esta situación. Por medio de expedientes de pacientes anonimizados de un centro de aborto flamenco, comparamos el número de solicitudes y abortos durante el primer cierre (16 de marzo al 14 de junio de 2020) con el mismo período en años anteriores. Utilizando un enfoque fenomenológico, documentamos los procedimientos y realizamos entrevistas (todas codificadas por inducción en Nvivo) con el coordinador del centro, siete integrantes del personal psicosocial y tres médicos. Aunque menos personas solicitaron y tuvieron un aborto, el personal estaba bajo mucha presión debido a los cambios en procedimientos. Un cambio sustancial fue sustituir las consultas telefónicas por consultas presenciales, las cuales el personal percibió como menos adecuadas para discutir preocupaciones, brindar consejería sobre anticoncepción y generar confianza. El centro permaneció accesible, pero el personal percibió una influencia en las reacciones emocionales de las usuarias. Aunque el personal estuvo de acuerdo en que el cierre no influyó de manera negativa en el procedimiento de aborto en sí, sintió una influencia negativa en el nivel de apoyo psicológico que podía ofrecer, especialmente en interacciones con usuarias que estaban menos seguras de su elección y usuarias con quienes no tenían un idioma en común. Cuando se relajó el cierre, se estableció un sistema de triaje para garantizar servicios de aborto emocionalmente seguros, según la percepción del personal, para todas las usuarias.
Background
From 14 March 2020, the Belgian government enforced a national lockdown to control the spread of COVID-19. Schools, restaurants, and non-essential shops were closed, working from home was encouraged, and people were urged to stay inside. Leaving the house was only permitted for essential activities or limited outdoor exercise with close family or one friend. On 10 May, measures were relaxed.
The COVID-19 outbreak and the protective measures implemented by the government had a significant impact on primary health care within Belgium, with changes in practice management and consultation strategies (e.g. tele-consultations) quickly being adopted.Citation1,Citation2 Researchers in other countries point to a significant influence on sexual and reproductive health (SRH) services, including abortion services.Citation3–9 The WHO also warned of possible negative effects of disrupted SRH services, and advised ensuring safe abortion care to the full extent of the law by considering barriers that could delay care, investing in medical abortion, implementing telemedicine-based solutions, and anticipating the increased need of certain medications.Citation10 However, since abortion is still an intensively debated practice, it is not surprising that countries have reacted to these challenges in different ways.Citation5,Citation6 While some countries (e.g. Poland and Malta) legally or practically restricted the possibilities for abortion under the guise of COVID-19,Citation5,Citation6 others (e.g. The Netherlands and Austria) did not, but chose not to counteract new barriers emerging due to COVID-19,Citation6–8 and yet others (e.g. Great Britain and France) legally or practically relaxed regulations (at least temporarily), thereby giving potential clients more autonomy.Citation6,Citation9
To date, only a few studiesCitation11–14 have empirically examined the influence of either the pandemic generally, or the measures of the first lockdown on SRH services and abortion care. These studies show that clients encountered more difficulties in obtaining (timely) SRH servicesCitation11 and that there was an increase in the demand for self-managed abortion among people living in countries with strict COVID-19 regulations,Citation12,Citation13 but also suggest that alternative services, such as self-managed abortion and telemedicine, were well received.Citation14
Furthermore, to the best of our knowledge, there is still no research addressing healthcare workers’ experience with delivering abortion services during COVID-19. COVID-19 precipitated an unexpected trial period in which abortion service providers had to quickly make changes in the way the abortion procedure was organised and comprehensive abortion care was offered, changes that might otherwise have been the topic of elaborate and prolonged debates. It therefore offers a unique opportunity to investigate a sudden turnaround in the organisation of abortion care, something that would otherwise have remained at the theoretical level. Our research aims to do this by researching the impact of COVID-19 measures on the abortion service in Flanders, Belgium, through the eyes of the abortion centre’s staff.
To this end, this study presents information on how, within the Belgian context, abortion care (defined as the entire process a client and the centre progress through together: from the first contact to the option for after-care) was organised usually, and during the first COVID-19 lockdown. Data were obtained from anonymised patient records and through in-depth interviews with staff members from an abortion centre in a medium-sized Belgian city. We aimed to (1) identify differences in the prevalence of abortion requests and actual abortions during the lockdown, (2) map out the regular and adapted abortion service procedures, (3) describe how the staff experienced the implementation of the COVID-19 measures and its perceived influence on their professional functioning, on the quality of the services, and on the client’s experience, and (4) identify what lessons can be learned from this unexpected change in procedures.
Context
Comparative statisticsCitation15 show that the Belgian abortion ratio of 152 abortions per 1000 live births is below the European Union average but similar to that of neighbouring countries. In Belgium, in accordance with the 1990 Law on the Termination of Pregnancy, abortion is available on request during the first 14 weeks of gestation. A mandatory six-day waiting period is in place. Abortions must be performed by a physician in a hospital or a licensed abortion centre. Self-managed abortions are illegal and could lead to prosecution. In Flanders, where this study is located, abortions due to medical complications (also allowed after 14 weeks of gestation) are performed in a hospital, while abortion on request is organised through the LUNA clinics, a non-profit network of five non-hospital-based abortion centres. LUNA performs approximately 97% of all registered abortions in Flanders (numbers from 2017).Citation16
Obtaining abortion care at one of the LUNA centres typically consists of clients or their social or healthcare worker calling the centre. Usually, an appointment is obtained within 10 days. Two appointments are required: the first one in which the abortion request is explored and a medical examination occurs, and – after the mandatory six days waiting period – a second appointment in which the pregnancy termination is initiated, either by undergoing a curettage or by taking mifepristone. In the case of a medical abortion, clients have to return a third time the next day to take misoprostol, after which they stay for a three-hour observation period. A follow-up appointment is possible, but not obligatory. Abortion care is almost entirely covered by public health insurance for all Belgian residents, with out-of-pocket costs restricted to €3.68 per abortion.
Method
We intensively studied one abortion centre, located in one of the bigger Flemish cities, which implemented strict COVID-19 protective measures between 16 March and 14 June 2020 (hereafter referred to as the lockdown).
To contextualise, we used anonymised patient records from this centre to compare the number of abortion requests and actual abortions during the lockdown with the numbers from the same period in the preceding years (2015–2020, hereafter referred to as the reference period).
To explore the impact of the COVID-19 measures on the experience of the abortion staff, a phenomenological approach was used. We mapped out and compared the usual abortion service and the abortion service during the lockdown through documents and meetings with the coordinator. We also present data from semi-structured in-depth interviews with the centre’s staff concerning their experience of these changes.
Apart from the coordinator and the doctors, all staff members fulfil the same functions (administrative tasks, occupying the reception, conducting intake consultations, giving contraceptive counselling, etc.), the only difference being that those who have a nursing or midwifery degree are also allowed to assist the doctors. These staff members are referred to as “psychosocial workers”, and are indicated with the letter “P” in quotations below. The coordinator of the centre was also trained as a psychosocial worker and still fulfils this function when extra help is needed. Quotations that originated from a doctor are indicated with the letter “D”.
We interviewed 11 of the 14 staff members of the centre (two refused and one was unavailable during the period of data collection). provides an overview of the function and gender of all staff members and of those interviewed. Eight of these interviews took place during the lockdown (between 1 May and 8 June) and were organised through a secure online platform. These interviews focused on the difference between the reference and the lockdown period. Three additional face-to-face interviews were conducted after the lockdown, at the end of August 2020. In these interviews, participants were asked to recall what they experienced during the lockdown, which might have caused some recall bias. However, they were also able to reflect on how the procedures evolved after the lockdown.
Table 1. Count of staff members that were interviewed versus all staff members employed at the abortion centre by professional status and gender
All interviews were transcribed verbatim, inductively coded, and analysed with NVivo software. The interviews were conducted in Dutch and the original Dutch transcripts were used for the analysis. In the English translation of the quotes used in this paper, we tried to stay as close to the participant’s language as possible.
The topic list used in the interviews covered the adaptations that were made in order to comply with national and local COVID-19 protective measures, the staff’s evaluation of these changes, and how staff perceived the influence of these measures on their professional and emotional functioning and on the client’s experience. Informed consent was obtained from all participants included in the study, and ethical clearance for this study was obtained from the University of Antwerp’s Ethics Committee for the Social Sciences and Humanities (reference number: SHW_20_22).
Results
Changes in the prevalence of abortions
During the lockdown, there were fewer abortion requests (596) than in the reference period (average 733.8) (). The same was true for the number of actual abortions (501 during the lockdown compared to an average of 615.4 in the reference period). The percentage of clients who had a first consultation but did not receive the actual procedure did not differ substantially between the lockdown and the reference period. The number of curettages slightly dropped from an average of 524.0 during the reference period to 490 during the lockdown. However, only 11 medical abortions happened during the lockdown, which is in sharp contrast to an average of 91.4 medical abortions during the reference period (see ). In the referral hospital in which medical abortions were possible during the lockdown, the number of medical abortions slightly increased (from 69.8 on average between March and June in the reference period to 86 during the lockdown).
Figure 1. Minimum, maximum, and average number of abortion requests, abortions, and type of abortion during the period of lockdown compared to the reference period
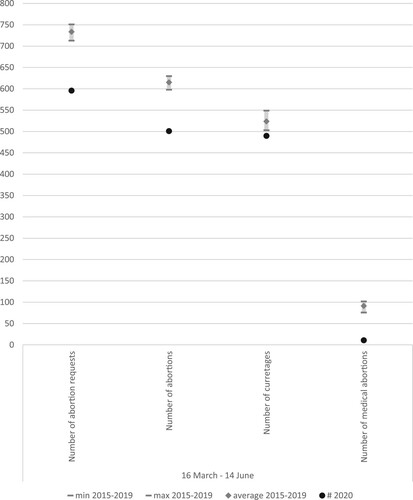
Table 2. Clients who request an abortion versus clients who actually receive an abortion during the period of lockdown compared to the reference period
Changes in the procedure and influence of COVID-19 protective measures on staff and clients as perceived by the staff
Anticipating a national lockdown, the abortion centre pro-actively developed a new procedure (within the limits of the national COVID-19 guidelines) to keep the service accessible and safe (concerning both the procedure and the virus). This new procedure was developed independently from other abortion centres and was approved by the National Institute for Health and Disability Insurance (RIZIV). Next to tightening hygiene procedures (frequent cleaning of high-touch areas, compulsory mask-wearing by both staff and clients, installing Plexiglas screens in the reception area), the centre minimised close in-person contact between staff and with clients. presents a general overview of the most important changes between the abortion service procedure before and during the lockdown.
Figure 2. Overview of the changes made in the abortion procedure due to COVID-19 protective measures
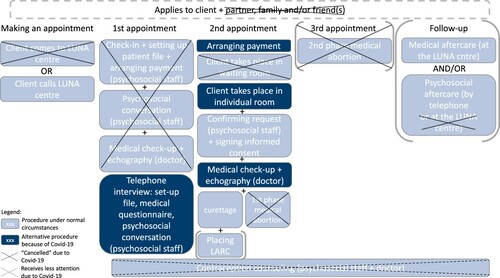
The following section discusses the abortion service procedure phase by phase, in each phase first describing the usual procedure, then the altered procedure, and finally, how the staff perceived the influence of these changes on themselves and the clients.
Making the first appointment
Usually, clients book the first appointment over the phone or visit the centre. During the lockdown, appointments could only be made over the phone. If clients did present at the abortion centre, they were turned away and asked to make a telephone call instead.
The abortion centre worked hard to keep their services safe and available during the lockdown, but might not have realised that potential clients were not aware of this. Clients who were sent home to make an appointment by telephone might have felt annoyed by the unnecessary trip and the associated costs (e.g. train tickets) and arrangements (e.g. childcare). However, this rarely happened. More striking was that during the first telephonic contact, the staff noticed that clients voiced the fear that the abortion services were compromised because of COVID-19. However, the staff also mentioned that clients expressed relief when finding out that they could continue to seek abortion care during the lockdown, and that most clients appeared to be understanding about the new procedures.
First appointment
The usual procedure for receiving abortion care encompasses either two obligatory visits to the abortion centre – in the case of a curettage – or – in the case of a medical abortion – three visits. Clients are allowed to bring someone along for practical reasons (e.g. as translator) or for emotional support.
During the first appointment, clients first register at the reception and sign health insurance papers. Next, they are directed towards the shared waiting room, where they complete a medical questionnaire.
A psychosocial staff member then receives the client in a private room where they discuss the unwanted pregnancy circumstances, possible doubts and questions, and previously used and planned contraceptives. After this, the client visits the doctor for a medical examination. The doctor consults the completed medical questionnaire, performs an ultrasound, informs the client about the pregnancy characteristics, and discusses the options for the procedure and future contraceptive use. The ultrasound is required because the doctor needs to confirm and register the precise gestational age. However, clients are informed during the psychosocial conversation that the screen and sound are not shared, unless the client requests this.
Finally, if the client decides to continue with the abortion, the procedure is scheduled after a compulsory six-day waiting period. If a client is still in doubt, or if there is a need to talk more, another appointment can be booked, or the client can be referred to a psychologist, a family-planning chat-line, or other relevant professionals.
In the altered procedure, the first consultation was replaced by a telephone interview conducted by staff members from their homes. This enabled the abortion centre to limit in-person interactions between staff members. Many aspects of the in-person interview were no longer possible, such as signing paperwork, or moderating the presence of other persons in the room. Therefore, clients were asked to avoid including family or friends in the call, and the signing of paperwork was postponed to the second appointment. While the doctor usually reviews the medical information, this task was also included in the telephone call with the psychosocial worker. During this first consultation, there was no contact with a doctor (unless necessary), nor was there the possibility to perform an ultrasound, which was postponed to the second appointment. Due to time constraints linked to the re-organisation, the staff’s learning curve to adapt to the new procedures, and colleagues falling sick or being placed in quarantine, it was decided to prioritise helping as many clients as possible above giving elaborate support to some clients with more psychosocial needs. The latter group was referred to a partner organisation that provides information and counselling concerning pregnancy choices.
The staff members indicated that these changes in the procedure had several consequences. Postponing the signing of paperwork resulted in an increased financial burden for the abortion centre. If the client did not make or show up for the second appointment, they could not sign the paperwork, meaning the abortion centre would lose financial compensation for the first appointment. The centre did try to contact clients by phone and send them the paperwork, but this solution regularly failed.
Staff members found the telephone consultations more challenging than face-to-face conversations. Because of the absence of non-verbal cues over the telephone, staff members found it challenging to assess the client’s emotions and personal situation accurately and build trust with the client. This made staff members more insecure, and, as a consequence, they had the feeling that they were less probing in the telephone interviews.
“If I would have had that woman in front of me, she might have cried. But on the telephone, it doesn't happen like that. In some way, it is more superficial or more business-like. Also, because you are doing this medical questionnaire […], you are in a situation with closed questions […] if then you start asking […] ‘What is it like for you to make this decision?’, that's suddenly a strange change in the kind of conversation. […] That causes the telephone interview to be more superficial sometimes.” (P4)
The contraception counselling suffered from these same hurdles and therefore received much less attention. Visual tools, which are particularly useful to discuss this topic, could no longer be used. Hence, the telephone consultations were reduced to the essence: they were much shorter than “normal” face-to-face interviews and more focused on practical and technical issues. Many staff members felt that this had a negative influence on their ability to “care” for the clients.
“If someone is sitting in front of me, and I see that she is fighting against her tears, then I know ‘this is difficult’. But if you don't see that on the phone, then you miss certain things. And then if people don't tell you because … yeah, you're talking to a stranger, then those things don't come to the surface. So in this respect, we had the feeling that we're not giving the support that we otherwise give when somebody is sitting in front of us.” (P8)
“Language is always a problem. But because of the lack of physical contact, because you can't explain things with hands and feet, because that often happens, that makes it even more difficult. […] You notice how that hurdle becomes taller and taller because of the telephone interviews.” (P1)
“Since the relaxation we partially have telephone consultations and partially consultations in the centre, in order to limit the amount of people in the waiting room. And we see that there are many more people who request a consultation in the centre than that there are people who request a telephone consultation. […] We thought, ‘Many people will be happy that they don't have to come here to have this conversation, that it can happen instead via telephone, that they don't have to come all the way.’ But no.” (P8)
Second appointment
During the second appointment, clients usually come to the centre and register at the reception desk. Clients who come for a curettage take a place in the waiting room together with their entourage, until they are assigned an individual room. Here, they have a consultation with a psychosocial staff member in which they can ask additional questions, future contraception can be discussed, and in which the client’s wish for abortion is confirmed. Clients will also be asked to sign an informed consent form. After this, clients are brought into the doctor’s office (alone or with a supporting person). The doctor performs a quick check-up and a second ultrasound. Clients were asked to take preparatory medication (for which they receive a prescription at the first appointment) vaginally at home, three hours before the procedure. At the centre, a doctor, assisted by a psychosocial staff member qualified to give medical assistance, performs the abortion procedure. In cases where this was requested by the client, the doctor also places a long-acting contraceptive device. After the procedure, the client can rest in an individual room. The doctor will check on the client some time later and give information concerning aftercare. A follow-up appointment can be made if needed. Afterwards, the client is discharged. In the case of a medical abortion, the client is directed straight from the waiting room to the doctor’s office (unless the client first wants to discuss questions or worries with a psychosocial worker). In this case, it is the doctor who will confirm the wish for abortion and ask the client to sign the informed consent form. After the medical examination and ultrasound, the client takes the abortion medication (mifepristone) under the staff’s supervision and is asked to come back the next day in order to take the second medication, misoprostol (see the third appointment).
In the altered procedure, clients were asked to sign the informed consent at the reception desk. A maximum of one supporting adult (no children) was allowed. Both staff and clients were asked to wear facemasks at all times. Furthermore, to limit in-person contact, clients were not taken to the waiting room but were immediately directed towards a private room. Clients were then called into the doctor’s office, but guests were not allowed to join. Previously, clients had the choice between a medical abortion and a curettage. However, in Flanders, a medical abortion requires the client to come to the abortion centre for taking both mifepristone and misoprostol. After taking misoprostol, clients are required to stay at the abortion centre for approximately three to four hours before going home. Therefore, it was decided not to offer medical abortions during the lockdown. Clients were informed about this limitation during their telephone interview. For those clients who did not want to change to a curettage, the abortion centre made an agreement with a nearby hospital to which clients could be referred for a medical abortion. This meant that almost all abortions in the abortion centre during the lockdown were curettages.
Due to the switch to telephone interviews, clients had not yet received an ultrasound and did not receive premedication to take (vaginally) at home. They therefore received the ultrasound at this point, and were asked to take the premedication sublingually. Clients were then returned to the private room, where they waited for one hour to allow the medication to start working. During this waiting time, they would receive a visit from a psychosocial staff member. After an hour, the doctor performed the procedure and placed long-acting contraception if this was requested. Afterwards, clients could take a short rest in the private room, but they were asked not to use the bed (in order not to lose too much time disinfecting the bed). Finally, the client was discharged.
Again, staff members indicated that these alterations in the procedure might have resulted in several consequences. They had the impression that fewer clients than usual showed up at the second appointment. They saw this as a consequence of two things. First, this may have resulted from the more business-like first appointments over the phone, and the associated risk that not all information came across correctly to the client, particularly in clients who were not fluent in one of the local languages. Second, staff members had the impression that clients enquired about the possibility of abortion care at earlier gestational ages during the lockdown. This could mean that there was still a high chance of having a miscarriage between the first and second appointments. Because few clients confirm their pregnancy with a gynaecologist, and home-tests are less reliable or misinterpreted, a group of these clients may not have been pregnant at all. The staff members assumed that this could explain why some clients do not present after making an appointment.
Compared to pre-COVID circumstances, staff members perceived some clients to be more stressed, worried, and/or emotional during the second appointment. Few of these worries appeared to be COVID-19-related, other than possible suspension of abortion services, reinforcing the staff’s perception that the telephone consultations were less accommodating for discussing worries and doubts and building trust. In addition, the staff had the impression that because clients were no longer able to get familiar with the abortion centre during their first appointment, they carried nervous feelings with them until the day of the procedure. The staff was of the opinion that this can lead to overwhelming emotions.
“Of course, the women who come here for the first time, those who had their psychosocial conversation on the telephone, they have a different bond with the centre. And you feel that. Because many women also wonder ‘where will we end up?’, ‘What is that place going to be like?’, they still have prejudices about abortion and abortion doctors, and when they arrive here and they see the nice rooms, decent furniture, nice tools, yeah, people walking around in medical uniforms, then they are reassured.” (D2)
“With COVID, now when there are emotions, they emerge during the procedure or right before. Otherwise this happens in your first conversation, you have mostly covered this. […] But now that happens less. Mainly the doctors notice this. That they are suddenly confronted with more emotions, because otherwise we are the ones that have mostly taken this away. And that is [the result of] the phone and the fact that women haven't been here in the centre yet.” (P7)
“They then also have that first confrontation, the ultrasound, ‘How long have I been pregnant?’ Sometimes the pregnancy term matters. So normally all of this can already rest for a week. Also other news, such as that it is a double pregnancy, or if you hear ‘I’m already 12 weeks and I thought I was only 6 weeks far’, or ‘I am longer than 14 weeks pregnant and I can’t be helped here anymore.’ Yeah, that is of course … different than when you can do this at the first appointment and have more time. Where people let these first emotions from the doctor’s office rest a bit more.” (P5)
“Also medically it was sometimes difficult […] you used to have two contact moments, as a doctor, you had the time and space to investigate uncertainties. Now, because of COVID … you couldn’t do that. […] If you were not sure, you had to disappoint a patient and tell them ‘you have to go home without receiving the procedure’, so you don’t want to do that, but on the other side you had to be strict for your own working mechanisms and say ‘I do not feel safe as a doctor, I do not want to perform this procedure now, I need space and time to plan this further.’ So yes, that caused a lot of stress.” (D3)
“These people never see our faces. We are completely covered with a mouth-nose mask. And I notice that, for sure. I think I am very mimetic, or convey a lot with my face, and now that’s not possible or it is difficult. And I have the idea that it is a lot more difficult for me to reassure people from behind this mask.” (P2)
Lastly, the new way of organising ultrasounds and curettages meant that the doctors had to “experiment” with a different way of delivering the premedication. For example, they found that when administering the premedication sublingually, it was effective after only one hour (instead of three) and had a better effect on the body. This improved therapy compliance and in the future may result in fewer schedule changes due to clients who took their medication too late. Both doctors and psychosocial staff members mentioned that they would like to keep this altered procedure after the lockdown.
Third appointment
When clients choose to have a medical abortion, they are asked to come back for a third appointment to receive the medication that evokes the expulsion of the pregnancy (misoprostol). Clients then have to stay for several hours so that the staff can check whether problems (such as excessive bleeding) arise. Many clients are nonetheless sent home while the expulsion is not yet complete. Therefore, clients are discouraged from having a medical abortion if they cannot count on support at home.
Because the abortion centre chose not to offer medical abortions during the lockdown, this phase was not present in the altered procedure. However, not all staff members agreed with this decision. Some thought that the centre should have taken the lockdown as an opportunity to find out how to offer medical abortions at home safely. After the national COVID measures were relaxed, the centre decided to take this step. Clients who preferred to have a medical abortion were asked to come to the centre for their first consultation to have an ultrasound and find out whether they were eligible for a medical abortion. For their second appointment, clients also came to the centre to take the mifepristone, and they received the misoprostol, which they were allowed to take at home later. On this day, there was telephonic contact between the centre and the client to follow-up on how the expulsion was progressing. For the staff, the experience of offering medical abortions at home with telephonic guidance resulted in feeling very positive. Therefore, the centre hopes to continue to offer this option, also after COVID-19.
“It’s better if people can do the medical abortion at home. […] We came to the conclusion that sitting here and waiting for the expulsion does not make any sense. […] because of the fact that you’re not so focused on the waiting for the expulsion, the body relaxes better and everything goes more smoothly.” (D3)
Follow-up appointment
The abortion centre also offers aftercare (medical check-ups and for psychosocial support) if required or wanted, but in general, the abortion centre does not receive many requests.
During the COVID-lockdown, aftercare was preferably done by telephone unless there was a medical need to come to the centre. The number of requests for aftercare did not change much because of the COVID-19 situation, and staff members did not mention any issues related to aftercare.
Working conditions during the lockdown
Usually, the psychosocial staff members of the abortion centre have a rather varied set of tasks: they perform administrative tasks, function as receptionists, conduct psychosocial interviews, provide contraceptive counselling, and some are also trained to assist with medical tasks. Typically they perform several different tasks each day and never perform the same task all day long.
The altered abortion service procedure required a very different general workflow. This mainly affected the psychosocial staff. To be able to work from home as much as possible, limit in-person contacts, and make it possible to master the new procedures as quickly as possible, tasks were redistributed in a manner that allowed for much less variety. Staff members had to perform the same task for a day or more at the end. Additionally, all formal staff meetings and training were cancelled, and informal ways of transferring information were limited.
Staff members mentioned that it was not easy for everyone to get used to the altered workflow, which could be frustrating. Not being able to see colleagues and having communication limited to mostly dry, to-the-point information exchanges made some staff members feel lonelier and less secure.
“What also changes […] is that you see your colleagues a lot less […] because several people are working from home. […] A certain conversation can have a certain gravity […] We used to have the chance to immediately vent about this if it was necessary, but also just to consult. […] If you’re unsure about which way to go, then you could always immediately discuss this with colleagues in pre-COVID times. And of course you don’t have that when working from home.” (P6)
“I have the feeling that now […] I can’t grasp many aspects of peoples’ stories. That many things are left unsaid now. Just out of necessity, because we, yeah, we have to spend that attention more to other things, to hygiene measures. We are disinfecting at 100 per hour.” (P6)
General appraisal of the adapted procedure by the abortion staff
Staff members expressed that the COVID-19 situation yielded a unique position in which, despite the challenges, there were also learning opportunities.
“I think that COVID also yielded many new insights, but it also installed a trial period in which we could try things in different ways. […] … it made us aware of good things, but also of things that were less good. […] Now we are in the phase in which we can say ‘Now, we’ll draw conclusions. Now we’ll see what to keep from what period’.” (D3)
“Of course the work is nicer in non-COVID times, but I think that the quality in these circumstances has stayed very high. […] You thought ‘Wow, working in those circumstances is not possible!’, but then you notice that it IS possible.” (D1)
“It gives you the feeling that Okay, we do offer a correct service, but euhm, we would prefer to start ‘caring’ for someone again.” (P4)
“We always have the trade-off between ‘offering enough’ and ‘not wanting to offer too much’. In order to also leave people in their strength. And I think that in the end, most people reacted very well to this situation. […] We have to realize that pampering is also not always necessary. People can get through this procedure from their own strength. And maybe we need to appeal to that strength rather than think that we have to solve everything with our services to support them as well as possible. That is often a very paternalistic attitude.” (P6)
Discussion
This study aimed to (1) identify differences in the prevalence of abortion care during the lockdown, (2) map out the regular and adapted abortion service procedures, (3) describe how the staff experienced the implementation of the COVID-19 measures and its perceived influence on their professional functioning, on the quality of the services, and on the client’s experience, and (4) identify which lessons can be learned from this unexpected change in the procedures. Our study comes to a number of main conclusions.
First, we established that there were fewer abortion requests and actual abortions during the first COVID-19 lockdown in Flanders than in the same period in the previous years. This could mean that there were fewer (unwanted) pregnancies, for example, because the economic, psychological, and social consequences of COVID-19 caused a decline in sex drive.Citation17 Additionally, as shown by Lindberg and colleagues,Citation11 the COVID-19 situation might have made people more aware of the need for good contraception, which potentially led to more careful and consistent contraception use. The fear of the virus and/or the imposed restriction of social contacts might also have resulted in less sexual risk-taking.Citation17 However, it could also reflect a real (e.g. inability to leave the house without someone knowing, to find solutions for care responsibilities, financial problems) or perceived (e.g. fear of getting infected with the virus, thinking that abortion is not an allowed “necessary” travel) barriers that arose due to COVID-19. Furthermore, the estimated increase of intimate partner violence (IPV) during COVID-19 might have complicated the process of seeking abortion care. Future research should aim to identify if there was more unmet need concerning abortions during the lockdown. Staff members had the impression that clients were surprised (and relieved) that the abortion centre was open. Therefore, abortion centres, social and healthcare institutions, and governments could increase efforts to spread the word to the general public that abortion care services are still available.
Second, staff members expressed gratitude for the fact that they were able to keep on working during the lockdown, but also expressed feeling stressed, tired, and frustrated. Developing new procedures under major time pressure was stressful, carrying them out was tiring, and infrastructural problems (e.g. IT systems that were not adapted to working from home) brought on additional frustrations. Furthermore, the lack of contact between colleagues and the feeling that they could not be the caregivers they were used to being negatively influenced their job satisfaction. Preparing possible scenarios for emergency situations before they are predicted or expected to happen could ensure a swifter and less stressful roll out.
Third, the interviewed staff members agreed that while the technical and medical quality of abortions did not decrease during the lockdown, the changed procedures did influence the level of psychological support the staff was able to give, and both psychosocial staff and doctors also perceived an effect on the emotions displayed by the clients. Many of these observations were related to switching to telephone consultations. Currently, the international community is pushing telemedicine as an alternative for in-person abortion care.6,8, Citation18–20 Our study shows that while telemedicine would be a valuable additional option, in-person consultations should stay available, particularly when working with vulnerable clients, such as those who do not speak a common language, or who experienced conflicts, among others.
This observation is, however, based solely on the experience of the staff. As mentioned, the altered workflow was mentally and physically tiring for the staff, and impacted their ability to “be the caregiver they wanted to be”. This might have caused an augmented perception of clients’ emotions, and a bigger influence on the staff’s own feelings in return. Additionally, the perceived change in clients' emotions might also have been influenced by other COVID-19-related factors, such as the fact that they couldn’t bring an emotional support person or the “cold” atmosphere at the abortion centre (where everyone was wearing masks, clients were put in separate rooms, etc.).
It is clear that more research is needed to find out what the clients’ experience was. While a study in the UK indicated that clients’ satisfaction with telemedicine and self-managed abortions at home was high, only 13.7% of the clients who opted for this choice participated in the survey.Citation14 A large-scale survey from the Belgian Social Security Office also found the promising result that clients’ evaluation of telephone consultations was mostly positive, but this survey did not focus on abortion care and also pointed out that satisfaction was higher when clients were dealing with their regular care providers.Citation2 Furthermore, Belgian general practitioners were worried about the continuity of regular care for both acute and chronic care, and about the psychological and socioeconomic well-being of their clients.Citation1 On the other hand, although the staff had the impression that there was more attrition because of the tele-consultations, the patient records did not confirm this. For clients with mobility issues, clients who experience IPV, clients with less flexible work and/or childcare arrangements, among others, the fact that the COVID-19 situation required fewer in-person visits, might have reduced the burden of travelling to the abortion centre several times.
Finally, the COVID-19 pandemic forced the abortion centre into an unexpected experiment concerning how to organise abortion care in crisis times. While there were also challenges before COVID-19, staff members felt that several challenges were enlarged because of the restrictive measures. Staff members felt that the lack of personal contact with clients and the reduced time for contraception counselling and psychological support could negatively influence clients’ emotional reaction to the abortion, but they were also surprised by the strength that many clients demonstrated. Many clients seemed to be able to decide whether or not to have an abortion without much interference from the centre. This puts into perspective what abortion services should do versus what they could offer. Although only three interviews were held when the measures had been relaxed and clients were allowed to take misoprostol at home, the staff members that were able to reflect on this procedure evaluated it positively. The results of this study suggest that in the experience of the abortion staff, telemedicine and self-managed abortions at home could be included as options in the protocol for abortion care. In addition, the obligatory waiting time of six days could be replaced by a waiting time suited to the needs of the client. These changes would have a substantial impact on the options that clients have concerning abortion care, and should therefore also be evaluated from the clients’ perspective.
This study has several limitations. Because of the increased workload and work–family conflict among staff members during the COVID-19 pandemic, seeking respondents for this study was challenging. We therefore decided to focus solely on one abortion centre and to adjust our working methods when needed. Because all but three staff members were interviewed, the small sample size of our study did not hinder a thorough assessment of the studied abortion centre. However, in a national or global context, this means that our research needs to be seen as exploratory. Our findings cannot be extrapolated to other abortion centres within Belgium, particularly because these centres operate independently and developed their strategies to cope with the COVID-19 measures separately. It would be valuable for future research to study whether a different response in a very similar context yielded different or similar problems and opportunities. The strong emphasis on psychosocial support may possibly reflect the over-presence of psychosocial staff members in the abortion centre and in our sample. In addition, the interviews were partially conducted through a secured online platform and partially in-person (when the first lockdown measures were relaxed). While it was more difficult to build trust in online interviews, it was safer, and it gave the staff members more flexibility. However, respondents who were interviewed after the measures were relaxed, might have been influenced by recall bias.
Finally, our study only describes the perceived influence of the COVID-19 pandemic on abortion care from the staff members’ point of view. We did not interview clients, although this would unveil an important, different perspective on how abortion care was influenced by COVID-19. Future research should evaluate new procedures through the eyes of the clients.
Conclusion
This was, to our knowledge, the first European study to discuss the influence of COVID-19 on abortion services through the eyes of healthcare professionals. COVID-19 certainly raised barriers that posed challenges to the abortion centre (in balancing safety, efficiency, and accessibility), and its staff members (in ensuring their own physical and psychological safety while also wanting to guard the clients’ physical and psychological safety). Although the abortion centre was able to safeguard access to medically safe abortion care, offering extensive psychological and emotional support to all clients was perceived to be harder. In the staff’s experience, this possibly affected more vulnerable groups (such as people who speak different languages and people who experience conflicts concerning the abortion) to a greater extent. However, COVID-19 also brought the opportunity to experiment with and evaluate new procedures. In this regard, from the staff members’ perspective, the centre’s first experience with (partially) self-managed medical abortions at home was predominantly positive.
Acknowledgments
The authors would like to thank Françoise Dedrie and Sven Todts for facilitating the recruitment of interview participants, for providing data collected at the LUNA centre, and for comments that greatly improved the manuscript.
Authors’ contributions
Study conceptualisation and design, material preparation, data collection, and analysis were performed by Leen De Kort, who also wrote the first draft of the manuscript. Supervisors Sarah Van de Velde and Edwin Wouters reviewed and edited the manuscript.
Declarations
This study was funded by the University of Antwerp and was performed in line with the principles of the declaration of Helsinki. Approval was granted by the University of Antwerp’s Ethics Committee for the Social Sciences and Humanities (Ethische Adviescommissie Sociale & Humane Wetenschappen). The authors have no interests to declare that are relevant to the content of this article. Informed consent was obtained from all participants included in the study.
Additional information
Funding
References
- Verhoeven V, Tsakitzidis G, Philips H, et al. Impact of the COVID-19 pandemic on the core functions of primary care: will the cure be worse than the disease? A qualitative interview study in Flemish GPs. BMJ Open. 2020;10(6):e039674. doi:https://doi.org/10.1136/bmjopen-2020-039674.
- Intermutualistische enquete raadplegingen op afstand (NIC). (2020). In van het Rijksinstituut voor ziekte- en invaliditeitsverzekering. Available from: https://www.riziv.fgov.be/nl/themas/kost-terugbetaling/door-ziekenfonds/Paginas/zorg-afstand-wat-leren-eerste-ervaringen.aspx.
- Riley T, Sully E, Ahmed Z, et al. Estimates of the potential impact of the COVID-19 pandemic on sexual and reproductive health in low- and middle-income countries. Int Perspect Sex Reprod Health. 2020;46:73–76. doi:https://doi.org/10.1363/46e9020.
- Romanis EC, Parsons JA. Legal and policy responses to the delivery of abortion care during COVID-19. Int J Gynecol Obstetrics. 2020;151:479–486.
- Aly J, Haeger KO, Christy AY, et al. Contraception access during the COVID-19 pandemic. Contracept Reprod Med. 2020;5(1):17. DOI:https://doi.org/10.1186/s40834-020-00114-9.
- Moreau C, Shankar M, Glasier A, et al. Abortion regulation in Europe in the era of COVID-19: a spectrum of policy responses. BMJ Sex Reprod Health. 2020. DOI:https://doi.org/10.1136/bmjsrh-2020-200724.
- Caruana-Finkel L. Abortion in the time of COVID-19: perspectives from Malta. Sex Reprod Health Matters. 2020;28(1):1780679. DOI:https://doi.org/10.1080/26410397.2020.1780679.
- Cioffi A, Cioffi F, Rinaldi R. COVID-19 and abortion: the importance of guaranteeing a fundamental right. Sex Reprod Healthc. 2020;25:100538. DOI:https://doi.org/10.1016/j.srhc.2020.100538.
- Parsons JA, Romanis EC. 2020 developments in the provision of early medical abortion by telemedicine in the UK. Health Policy. 2020. DOI:https://doi.org/10.1016/j.healthpol.2020.11.006.
- World Health Organisation (WHO). (2020). Maintaining essential health services: operational guidance for the COVID-19 context. Available from: https://apps.who.int/iris/bitstream/handle/10665/332240/WHO-2019-nCoV-essential_health_services-2020.2-eng.pdf?sequence=1&isAllowed=y.
- Lindberg LD, VandeVusse A, Mueller J, et al. Early impacts of the COVID-19 pandemic: findings from the 2020 Guttmacher survey of reproductive health experiences. New York: Guttmacher Institute; 2020.
- Aiken ARA, Starling JE, Gomperts R, et al. Demand for self-managed online telemedicine abortion in eight European countries during the COVID-19 pandemic: a regression discontinuity analysis. BMJ Sex Reprod Health. 2020. DOI:https://doi.org/10.1101/2020.09.15.20195222.
- Aiken ARA, Starling JE, Gomperts R, et al. Demand for self-managed online telemedicine abortion in the United States during the coronavirus disease 2019 (COVID-19) pandemic. Obstet Gynecol. 2020;136(4):835–837. DOI:https://doi.org/10.1097/AOG.0000000000004081.
- Porter C, Lord J, Church K. (2020). Early medical abortion using telemedicine-acceptability to patients. medRxiv.
- World Health Organisation (WHO). European Health Information Gateway. Abortions per 1000 live births. [cited 2020 Oct 26]. Available from: https://gateway.euro.who.int/en/indicators/hfa_586-7010-abortions-per-1000-live-births/.
- Nationale Evaluatiecommissie Zwangerschapsafbreking (National Evaluation Committee on Pregnancy Termination). (2020). Nationale commissie voor de evaluatie van de wet van 3 april 1990 betreffende de zwangerschapsafbreking (wet van 13 augustus 1990) Verslag ten behoeve van het parlement 1 januari 2016–31 december 2017. [cited 2021 Feb 5]. Available from: https://overlegorganen.gezondheid.belgie.be/sites/default/files/documents/volledig_verslag_2018_nl_2020_1.pdf.
- Döring N. How is the COVID-19 pandemic affecting our sexualities? An overview of the current media narratives and research hypotheses. Arch Sex Behav. 2020;49(8):2765–2778. DOI:https://doi.org/10.1007/s10508-020-01790-z.
- Romanis EC, Parsons JA, Hodson N. COVID-19 and reproductive justice in Great Britain and the United States: ensuring access to abortion care during a global pandemic. J Law Biosci. 2020;7(1). DOI:https://doi.org/10.1093/jlb/lsaa027.
- Oyediran KA, Makinde OA, Adelakin O. The role of telemedicine in addressing access to sexual and reproductive health services in sub-saharan Africa during the COVID-19 pandemic. Afr J Reprod Health. 2020;24(2):49–55.
- Assis MP, Larrea S. Why self-managed abortion is so much more than a provisional solution for times of pandemic. Sex Reprod Health Matters. 2020;28(1):1779633. DOI:https://doi.org/10.1080/26410397.2020.1779633.